


Gallstones are collections of solid material (predominantly crystals of cholesterol) in the gallbladder.
The liver can secrete too much cholesterol, which is carried with bile to the gallbladder, where the excess cholesterol forms solid particles and accumulates.
Gallstones sometimes cause upper abdominal pain that can last for hours.
Ultrasonography is quite accurate in detecting gallstones.
If gallstones cause recurrent pain or other problems, the gallbladder is removed.
The gallbladder is a small, pear-shaped sac located beneath the liver. It stores bile, a fluid that is produced by the liver and aids in digestion. When bile is needed, as when people eat, the gallbladder contracts, pushing bile through the bile ducts into the small intestine. (See also Overview of Gallbladder and Bile Duct Disorders and figure View of the Liver and Gallbladder.)
Most disorders of the gallbladder and bile ducts result from gallstones. The risk factors for gallstones include the following:
Female sex
Older age
American Indian ethnicity
Obesity
Rapid weight loss (as results from a very low calorie diet or weight-loss surgery)
A typical Western diet
A family history of gallstones
In the United States, over 15% people age 60 to 75 have gallstones.
Stones in the gallbladder (also called cholelithiasis) sometimes pass into the bile ducts, or stones may form in the bile ducts. Stones in the bile ducts are called choledocholithiasis. These stones sometimes block a bile duct.
Most gallstones do not cause symptoms. But if symptoms or other problems occur, treatment is necessary. Each year, more than half a million people in the United States have their gallbladder surgically removed.
What Are Gallstones?
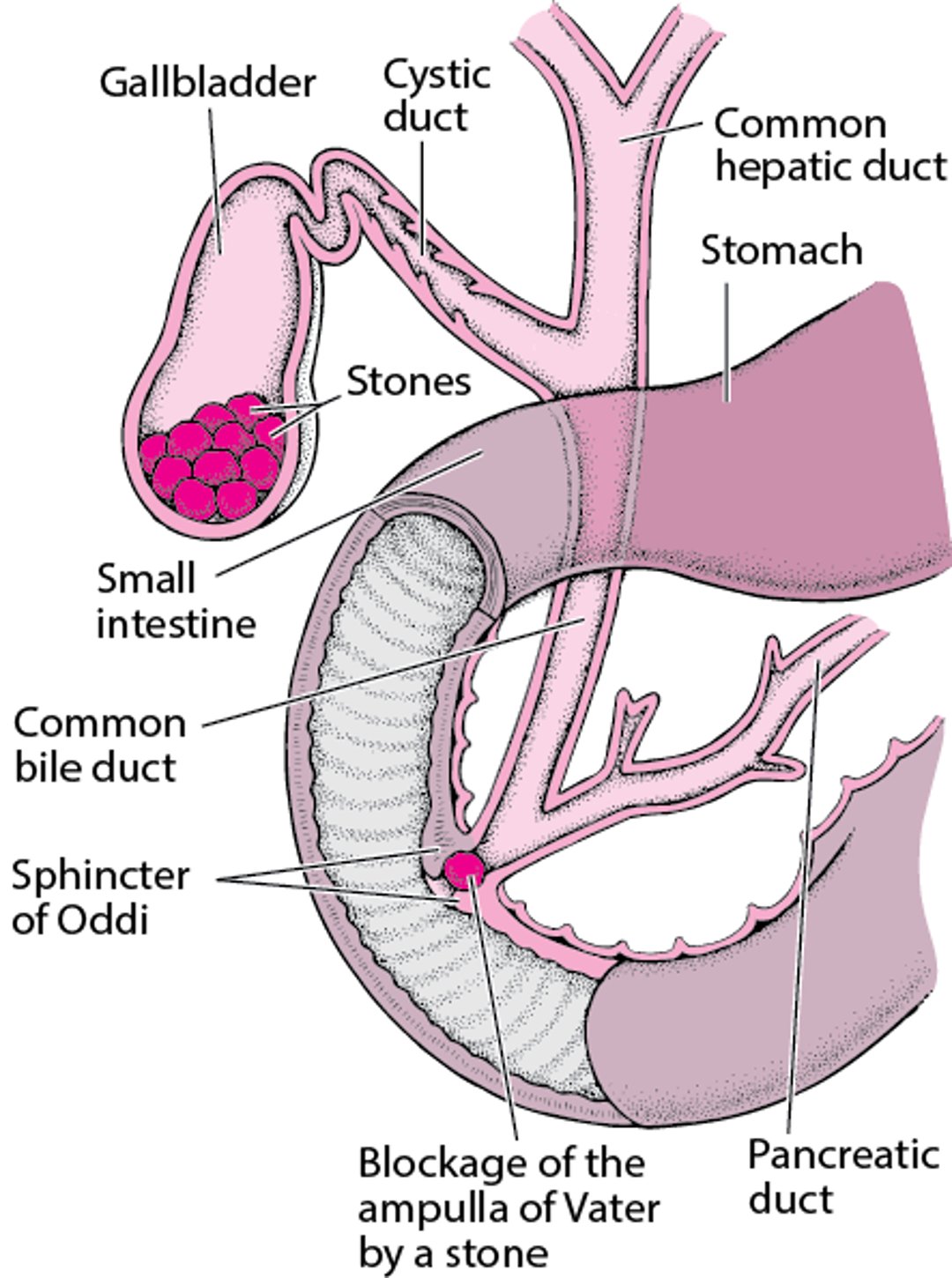
Gallstones are usually composed of cholesterol that has crystallized from bile. They form in the gallbladder. They may leave the gallbladder and lodge in the cystic duct, the common bile duct, or the ampulla of Vater. |

In the Western world, the major component of most gallstones is cholesterol, a fat (lipid) that normally is dissolved in bile (but not in water). When the liver secretes excess cholesterol, bile becomes oversaturated with cholesterol. The excess forms solid particles (cholesterol crystals). These microscopic crystals accumulate in the gallbladder, where they clump and grow into gallstones.
Other types of gallstones form in the same way, but the solid particles are calcium compounds or bilirubin (the main pigment in bile). Stones composed of bilirubin, called pigment stones, are either black (forming in the gallbladder) or brown (forming in the bile ducts). Black pigment stones are more likely to develop in people who have alcohol-related liver disease and/or cirrhosis, who are older, or who have hemolytic anemia (which occurs when the body destroys red blood cells prematurely). Brown pigment stones can form when the gallbladder or bile ducts are inflamed or infected or when the bile ducts are narrowed.
The stones may stay in the gallbladder or pass into bile ducts. Stones can block the cystic duct, common bile duct, or ampulla of Vater (where the common bile duct and pancreatic duct join). Most cholesterol stones in the bile ducts come from the gallbladder.
Any narrowing (stricture) of the bile ducts can lead to a blockage or slow bile flow. Bacterial infections can develop when bile flow is slowed or blocked.
Sometimes microscopic particles of cholesterol, calcium compounds, bilirubin, and other materials accumulate but do not form stones. This material is called biliary sludge. Sludge develops when bile remains in the gallbladder too long, as it does during pregnancy. Gallbladder sludge usually disappears when its cause resolves, for example, when pregnancy ends. However, sludge can evolve into gallstones or pass into the biliary tract and block the ducts.
Did You Know...
|
Symptoms of Gallstones
About 80% of people with gallstones do not have any symptoms for many years, if ever, particularly if the gallstones remain in the gallbladder.
Gallstones may cause pain. Pain develops when the stones pass from the gallbladder into the cystic duct, common bile duct, or ampulla of Vater and block the duct. Then the gallbladder swells, causing pain called biliary colic. The pain is felt in the upper abdomen, usually on the right side under the ribs. Sometimes the location is hard to pinpoint, particularly for people with diabetes and older people. The pain typically increases in intensity over 15 minutes to an hour and remains steady for up to 12 hours. The pain is usually severe enough to send people to the emergency department for relief. Once the pain begins to resolve, it does so over 30 to 90 minutes, leaving a dull ache. People often feel nauseated and vomit.
Eating a heavy meal can trigger biliary colic whether people eat fatty foods or not. Gallstones do not cause belching or bloating.
Although most episodes of biliary colic resolve spontaneously, pain returns in 20 to 40% of people each year, and complications may develop. Between episodes, people feel well.
If the blockage persists, the gallbladder becomes inflamed (a condition called acute cholecystitis). When the gallbladder is inflamed, bacteria flourish, and infection may develop. The inflammation usually causes fever.
Blockage of the common bile duct or the ampulla of Vater is more serious than blockage of the cystic duct. Blockage of a bile duct can cause the ducts to widen (dilate). It can also cause fever, chills, and jaundice (a yellowish discoloration of the skin and the whites of the eyes). This combination of symptoms indicates that a serious infection called acute cholangitis has developed. Bacteria can spread to the bloodstream and cause serious infections elsewhere in the body (sepsis). Also, pockets of pus (abscesses) can develop in the liver.
Stones that block the ampulla of Vater also can block the pancreatic duct, causing inflammation of the pancreas (pancreatitis), as well as pain.
Inflammation of the gallbladder caused by gallstones can erode the gallbladder wall, sometimes resulting in a hole (perforation). Perforation results in leakage of the gallbladder contents throughout the abdominal cavity, causing severe inflammation (peritonitis). A large gallstone that enters the small intestine can cause intestinal blockage, called a gallstone ileus. This rare complication is more likely to occur in older people.
Did You Know...
|
Diagnosis of Gallstones
Ultrasonography or other imaging test
Doctors suspect gallstones in people with the characteristic pain in the upper abdomen (caused by a swollen gallbladder). Sometimes gallstones are detected when an imaging test such as ultrasonography is done for other reasons.
Ultrasonography is the test of choice. It is 95% accurate in detecting gallstones in the gallbladder. It is less accurate in detecting stones in the bile ducts, but it may show that the blockage has caused the ducts to dilate. Other diagnostic tests may be necessary. They include
Magnetic resonance imaging (MRI) and computed tomography (CT) to check for stones in the gallbladder
Magnetic resonance cholangiopancreatography (MRCP) or, if MRCP is unclear, endoscopic ultrasonography (EUS) and/or endoscopic retrograde cholangiopancreatography (ERCP), to check for stones in the bile ducts
In endoscopic ultrasonography (EUS), an endoscope that contains a tiny ultrasound device at its tip is passed through the mouth into the stomach and the small intestine. It is positioned near the gallbladder and bile ducts and can show images of the structures there better than standard ultrasonography.
For ERCP, a flexible viewing tube (endoscope) with surgical attachments is passed through the mouth, down the esophagus, through the stomach, and into the small intestine (see figure Understanding Endoscopic Retrograde Cholangiopancreatography). A thin catheter is passed through the endoscope, into the opening between the small intestine and the common bile and pancreatic ducts and up into the common bile duct. A radiopaque contrast agent, which is visible on x-rays, is then injected through the catheter into the bile ducts, and x-rays are taken to detect any abnormalities.
Blood tests to evaluate how well the liver is functioning and whether it is damaged (liver tests) are done. Results are usually normal unless stones block the bile ducts. When stones block the bile ducts, results are usually abnormal, suggesting a backup of bile in the liver (cholestasis). Results often include an increase in bilirubin and in certain liver enzymes.
Treatment of Gallstones
Surgery to remove gallbladder (cholecystectomy)
Sometimes medications to dissolve gallstones
Sometimes gallstone removal via endoscopic retrograde cholangiopancreatography (ERCP)
Gallstones that do not cause symptoms (silent gallstones) do not require treatment. If gallstones cause pain, changing the diet (for example, to a low-fat diet) does not help.
Gallstones in the gallbladder
If gallstones cause disruptive, recurring episodes of pain, a doctor may recommend surgical removal of the gallbladder (cholecystectomy). Removal of the gallbladder prevents episodes of biliary colic yet does not affect digestion. No special dietary restrictions are required after surgery. During cholecystectomy, the doctor may also check for stones in the bile ducts.
About 90% of cholecystectomies are done using a viewing tube called a laparoscope. After small incisions are made in the abdomen, the laparoscope is inserted. Surgical tools are passed through the incisions and used to remove the gallbladder. Laparoscopic cholecystectomy has lessened the discomfort after surgery, shortened the length of hospital stays, provided better cosmetic results, and reduced the time needed to recover.
The rest of cholecystectomies are done by open abdominal surgery, which requires a larger incision in the abdomen.
Alternatively, gallstones can sometimes be dissolved with medications, such as bile acids (ursodeoxycholic acid), taken by mouth. Such a medication can dissolve tiny stones in 6 months. Larger stones may take up to 1 to 2 years. Many never dissolve. Dissolving gallstones with medications is most likely to work when stones are made of cholesterol and the opening of the gallbladder is not blocked. Even if the stones are successfully dissolved, half of these people develop gallstones again within 5 years. This treatment has limited use, and doctors primarily use it when surgery is too risky (for example, in people with major medical problems—see Surgical Risk).
Ursodeoxycholic acid, a medication taken by mouth, can help prevent stones from forming in people with obesity who are losing weight rapidly after weight-loss surgery or who are on a very low calorie diet.
Gallstones in the bile ducts
Most stones in the bile ducts can be removed during ERCP (see figure Understanding Endoscopic Retrograde Cholangiopancreatography). During this procedure, doctors pass an instrument through the endoscope and use it to cut the sphincter of Oddi (which is where the common bile duct connects to the small intestine)—a procedure called endoscopic sphincterotomy. Sometimes the end of the bile duct is also cut and widened. If the stones do not spill out into the small intestine on their own after the cut is made, a catheter with a small basket at its tip is inserted through the endoscope. It can be used to trap and then pull the stone out of the duct. Cutting the end of the bile duct leaves the opening wide enough to let any future stones pass more easily into the small intestine. Gallstones located in the gallbladder cannot be removed using this technique.
ERCP with endoscopic sphincterotomy is successful in 90% of people. It is far safer than open abdominal surgery. Fewer than 1% of people die from this procedure, but up to 7% experience complications soon after ERCP with endoscopic sphincterotomy. Such complications include inflammation of the pancreas (pancreatitis), and less commonly bleeding and perforation or infection of the bile ducts. Later on, in some people, the inflamed bile ducts narrow (called strictures). When the ducts narrow, stones are more likely to form in the ducts, causing more blockages in the ducts.
Most people who have had ERCP and endoscopic sphincterotomy later have their gallbladder removed, typically using a laparoscope. If the gallbladder remains, stones in the gallbladder may pass into the ducts, causing repeated blockages.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
International Foundation for Gastrointestinal Disorders (IFFGD): A reliable resource that helps people with gastrointestinal disorders manage their health.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Comprehensive information on how the digestive system works and links to related topics, such as research and treatment options.






